WP_Post Object
(
[ID] => 4831
[post_author] => 15
[post_date] => 2022-09-01 10:41:00
[post_date_gmt] => 2022-09-01 10:41:00
[post_content] =>
Here's what to read so you can get to know us better.
When I started The Conversationalist in 2018, I wanted to create a platform that amplified the voices of women and people of color with creative solutions and deep insights about this chaotic, interconnected world. There were too many critical stories that weren't getting the attention they deserved. The Conversationalist's mission was to build a feminist media outlet to publish these global perspectives, and to foster a space for readers to connect and engage over shared interests and concerns. We believed, and still do, that people are hungry for thoughtful, engaging journalism they can trust, a natural response to the proliferation of disinformation, propaganda, and equivocation over basic facts and human dignity. Curiosity and empathy thrive when the rage clicks disappear.
In pursuit of our goals, we decided to take a step back earlier this year so we could re-evaluate how to best honor our mission moving forward. And now, we're back. Just like before, we're prioritizing writers who shine a light on underreported stories and trends around the world. We plan to continue only publishing a couple stories a week for the time being, in pursuit of putting out fewer, richer stories rather than chasing clicks. But we're also thinking bigger: Feminism, at its core, is about linking the personal to the political, a critical commitment in times like these that demand human connection and collective action. It’s also about finding moments of joy, and with our relaunch, The Conversationalist aims to inform, connect, and delight. As you've noticed, we've fully embraced a new artistic direction, with the aim of supporting artists around the world, and are more committed than ever to celebrating human ingenuity and building community. I want to give a shout-out here to our Executive Editor, Gina Mei, whose editorial and creative vision for this relaunch has been a joy to witness, and the writers, artists, and countless other people who helped bring this new iteration to life.
As for our readers, we're so glad you're here. And in case you aren't already familiar with us, here are a few stories from The Conversationalist's archives—all hand-picked by the team—so you can get to know us a little better.
~
‘Bees are like my family’: A female beekeeper is reviving honey production in Kashmir Aliya Bashir / December 9, 2021
If you are looking for a sign to leave it all and start a new life as a beekeeper, look no further than this beautiful profile of Towseefa Rizvi and her family's apiary in Kashmir. It's both an honest look at the profession and the region, exploring the economic and cultural hurdles that keep women from beekeeping, while also showing why honey production can be a surprisingly accessible (and meaningful!) trade. Rizvi's deep love and care for her hive is contagious, and her dedication to sharing her knowledge with others is an absolute joy to read. It's a lovely and empowering piece, gorgeously reported by Aliya Kashir.
—Gina Mei
The fascism is already here, but we can’t see it through the lens of exceptionalism Anna Lind-Guzik / May 27, 2021
It’s maddening to watch a green-headed bird with webbed orange feet fly into your home, quacking wildly and gobbling up all your bread, only to be told, “That can’t be a duck; ducks live outside.” And it’s a relief when someone else notices the same things you’ve been noticing, and confirms that you’re not just being hysterical after all. That’s why I’d heartily recommend this story to anyone who’s worried about the future of U.S. democracy—if nothing else, it’ll reassure you that you’re not losing your mind.
—Nick Slater
Women are people, no matter what the Supreme Court says Raina Lipsitz / December 21, 2021
My picks follow a theme, which is, times that The Conversationalist’s contributors accurately, if unfortunately, foretold the near future.This article ran before Roe fell, and it remains both prescient and a great example of the solutions journalism The Conversationalist exists to elevate. “Anyone serious about defending the rights and dignity of all women needs to stop mourning and start confronting state power,” writes Lipsitz, and she’s right. Now that we’ve seen the full range of absurd Democratic leadership responses to Roe’s demise (Nancy Pelosi’s fundraising emails and Zionist poetry readings, my god) it’s beyond clear that no person of conscience can continue to perform “childlike deference to institutions that have outlived their usefulness, like the Supreme Court.” Americans may remain fundamentally uncomfortable with demanding accountability from their institutions, but this article is a great place to start contemplating what real domestic resistance could look like.
—Brenna Erford
A beginner’s guide to immigration Katie Dancey-Downs / March 10, 2022
Immigration vs. emigration vs. migration. What makes someone a refugee vs. an economic migrant? When it comes to immigration, things are more complicated than they may appear. In this beginner’s guide, Katie Dancey-Downs breaks it all down in a very digestible way. I love how approachable this makes the topic, but also how it answered all of my immigration questions I didn’t even think to ask yet. It includes history from some countries around the world (like Japan, Saudi Arabia, and the U.S., to name a few) and takes a look at where we stand today. This is a must-read for anyone looking to learn more about immigration and the motives behind why people seek out a new home.
—Kiera Wright-Ruiz
Russia as a mirror of American racism Kimberly St. Julian-Varnon / September 17, 2020
White supremacist movements are globally interconnected, which Kimberly St. Julian-Varnon demonstrates in this story on "Russian Lives Matter," a knock-off grassroots movement in Russia that borrowed the language of the American alt-right to promote white anti-Putin protesters and denigrate "Black Lives Matter" protests. American racism is one of our most dangerous exports, and an aspect of US influence that is taboo to mention in most mainstream coverage. I appreciate The Conversationalist's commitment to platforming writers who aren't afraid to take on sensitive, critical subjects with moral clarity and deep insight.
—Anna Lind-Guzik
Why you should continue to wear a mask outdoors, even after you’ve been vaccinated Jillian York / April 29, 2021
Confession: I was ready to hate this story based on the headline. But after a couple paragraphs it became obvious York was making a smart, nuanced point about adapting our behavior (in certain situations) to protect people who are vulnerable in ways we might not immediately recognize. It was a nice reminder to move through the world with more thoughtfulness and compassion. As someone who lives outside the U.S., I also appreciated the acknowledgement that other countries and other peoples exist—and everyone’s lives have meaning.
—N.S.
To stop Putin, grab him by his wallet Natalia Antonova / December 9, 2021
A scant two months before Russia invaded Ukraine and just four months before the US government imposed severe financial sanctions on Russia in response, The Conversationalist ran this damn-near-prophetic article by Natalia Antonova in which she makes a compelling case for the policy path the U.S. and numerous other nations ultimately followed. To defang Putin, Antonova argues that Western powers should leverage ordinary Russians’ contempt for the kleptocrats who comprise his inner circle—“that very justifiable hatred is one of Russia’s greatest vulnerabilities, and one of the saddest elements of modern Russian life, which is dominated by stress and suspicion.“ In service to this end, Western powers should create painful consequences for this circle via economic sanctions that target their opulent, offshore-stashed wealth. Additionally, she suggests targeting Russian private military companies, which the U.S. Department of State just recently moved to do in June of this year.
—B.E.
The Prodigal Techbro Maria Farrell / March 5, 2020
What can I say, I'm a sucker for a good headline, and the very concept of a "prodigal techbro" made me laugh—partly because Twitter has ruined my brain forever, but also because it's genuinely a clever moniker for the type of dude that Maria Farrell is describing. The piece takes a scalpel to the all-too-easy redemption arc of those who have left Big Tech and rebranded themselves as what might best be summed up as "good, actually." It's a nuanced take that acknowledges the importance of giving people second chances and allowing them to learn and grow from their mistakes; while also pointing out the many problems with immediately centering these folks in conversations and work that others have been having and doing for far longer.
—G.M.
Pakistani women are claiming their right to be in public spaces—one cup of chai at a time Anmol Irfan / March 26, 2021
I loved this story about Pakistani women who have started meeting up in public to drink chai, traditionally thought of as a men-only activity. It's a small but meaningful act of rebellion, as these women challenge patriarchal restrictions to their freedom of movement while enjoying a delicious cup of chai. It's also a story about class, as women from middle and upper class families have more opportunities to go abroad and get out of the house. As movement founder Sadia Khatri put it, "It took living in other countries to learn that I had been conforming to a clever scam my whole life, thinking the city belonged only to men."
—A.L.G.
[post_title] => Welcome to the "New" Conversationalist
[post_excerpt] => Here's what to read so you can get to know us better.
[post_status] => publish
[comment_status] => open
[ping_status] => open
[post_password] =>
[post_name] => welcome-to-the-new-conversationalist
[to_ping] =>
[pinged] => https://conversationalist.org/2021/04/29/why-you-should-continue-to-wear-a-mask-outdoors-even-after-youre-vaccinated/
https://conversationalist.org/2020/03/05/the-prodigal-techbro/
https://conversationalist.org/2021/12/21/women-are-people-no-matter-what-the-supreme-court-says/
https://conversationalist.org/2021/05/27/the-fascism-is-already-here-we-just-cant-see-it-through-the-lens-of-exceptionalism/
https://conversationalist.org/2021/12/09/bees-are-like-my-family-how-a-female-beekeeper-is-redefining-honey-production-in-kashmir/
https://conversationalist.org/2022/03/10/a-beginners-guide-to-immigration/
[post_modified] => 2024-08-28 21:14:02
[post_modified_gmt] => 2024-08-28 21:14:02
[post_content_filtered] =>
[post_parent] => 0
[guid] => https://conversationalist.org/?p=4831
[menu_order] => 115
[post_type] => post
[post_mime_type] =>
[comment_count] => 0
[filter] => raw
)





 Kashmiri children walking home from school in winter.[/caption]
Mental health experts and teachers report that the lockdowns have also exacerbated pre-existing physical and mental health problems, causing trauma that could take generations to heal.
Dr. Majid Shafi, a clinical psychiatrist who treats children and adolescents in the central and southern districts of Kashmir said restrictions on children, who are confined to their homes for long periods during extended lockdowns, has adversely affected their physical, emotional, and cognitive health.
“Almost every parent of kids and teenagers in Kashmir is complaining these days about increased behavioral issues in their children,” said Dr. Shafi, adding that he had seen an “appreciable increase” in symptoms such as a feeling of hopelessness, anxiety, mood disorders, and a decline in academic performance
Isha Malik, a clinical psychologist at a government-run children’s hospital in Srinagar, said the months-long suspension of phone and internet connectivity had severely hampered delivery of mental health-care services. As a consequence, she said, many of her patients had relapsed or seen their symptoms worsen.
Ms. Malik, who also treats psychosocial and mental health problems in children and women at her own clinic in Srinagar, said that drug abuse among adolescents has increased with the lockdowns because they could not “release their pent-up emotions” by meeting up with friends. Data collected by physicians at Kashmir’s Institute of Mental Health & Neurosciences (IMHANS)
Kashmiri children walking home from school in winter.[/caption]
Mental health experts and teachers report that the lockdowns have also exacerbated pre-existing physical and mental health problems, causing trauma that could take generations to heal.
Dr. Majid Shafi, a clinical psychiatrist who treats children and adolescents in the central and southern districts of Kashmir said restrictions on children, who are confined to their homes for long periods during extended lockdowns, has adversely affected their physical, emotional, and cognitive health.
“Almost every parent of kids and teenagers in Kashmir is complaining these days about increased behavioral issues in their children,” said Dr. Shafi, adding that he had seen an “appreciable increase” in symptoms such as a feeling of hopelessness, anxiety, mood disorders, and a decline in academic performance
Isha Malik, a clinical psychologist at a government-run children’s hospital in Srinagar, said the months-long suspension of phone and internet connectivity had severely hampered delivery of mental health-care services. As a consequence, she said, many of her patients had relapsed or seen their symptoms worsen.
Ms. Malik, who also treats psychosocial and mental health problems in children and women at her own clinic in Srinagar, said that drug abuse among adolescents has increased with the lockdowns because they could not “release their pent-up emotions” by meeting up with friends. Data collected by physicians at Kashmir’s Institute of Mental Health & Neurosciences (IMHANS) 
 Working as a pediatric emergency physician, Dr. Shaheen-Hussain saw the cruel consequences of the non-accompaniment practice first-hand in 2017, when he treated two young patients who were undergoing stressful medical procedures without their loved ones by their side. Quebec pediatricians had been demanding the end of this heartless practice for decades, but successive governments refused to change the policy, making Quebec an outlier in Canada. When a citizen confronted him about the matter at a public event in 2018 , Quebec’s then-Health Minister, Gaétan Barrette,
Working as a pediatric emergency physician, Dr. Shaheen-Hussain saw the cruel consequences of the non-accompaniment practice first-hand in 2017, when he treated two young patients who were undergoing stressful medical procedures without their loved ones by their side. Quebec pediatricians had been demanding the end of this heartless practice for decades, but successive governments refused to change the policy, making Quebec an outlier in Canada. When a citizen confronted him about the matter at a public event in 2018 , Quebec’s then-Health Minister, Gaétan Barrette, 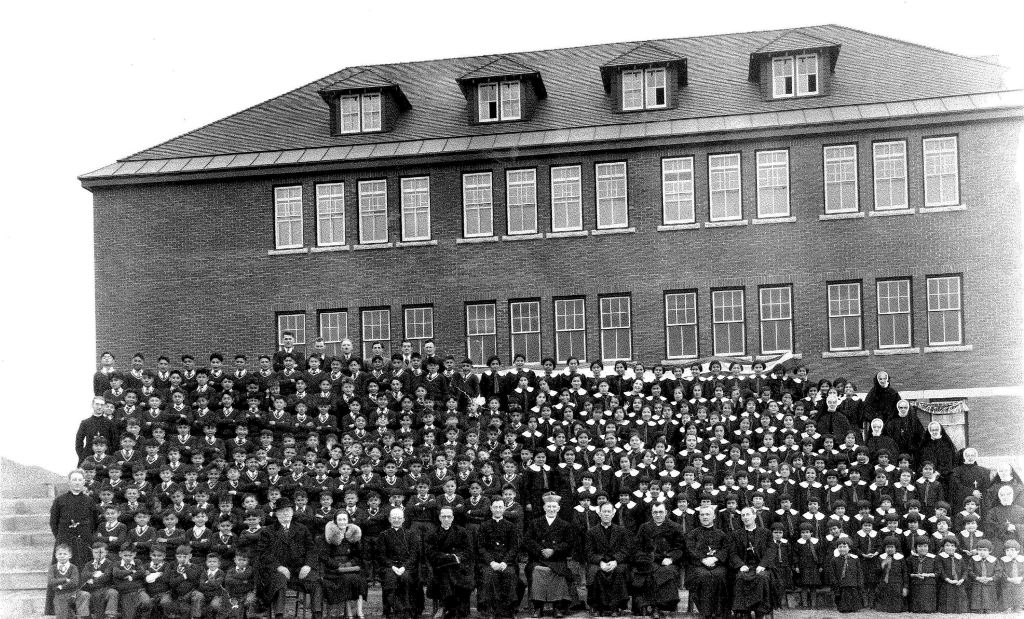 Kamloops Indian Residential School in 1937.[/caption]
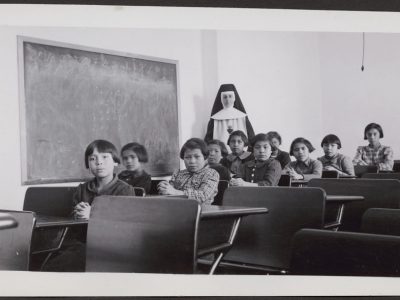
In addition, highly unethical
Kamloops Indian Residential School in 1937.[/caption]
In addition, highly unethical  A Black man is tested during the Tuskegee Study of Untreated Syphilis in the Negro Male.[/caption]
The
A Black man is tested during the Tuskegee Study of Untreated Syphilis in the Negro Male.[/caption]
The